US Measles Outbreak Passes 1,700 Cases but Shows Early Signs of Slowing
The US measles outbreak has exceeded 1,700 cases in 2026, with Utah as the new epicenter, but weekly case counts are beginning to decline.
Overview
The United States is navigating its most significant measles resurgence in decades. What began as localized clusters earlier in 2026 has expanded into a sustained, multi-state outbreak that has now surpassed 1,700 confirmed infections — a threshold not crossed in the country for many years. The outbreak has unfolded against a backdrop of declining childhood vaccination rates in some communities and an active public debate over vaccine safety that has reached the highest levels of federal government.
Measles is caused by one of the most contagious pathogens known to medicine. A single infectious individual can transmit the virus to nine out of ten unvaccinated people in close contact. The disease spreads through respiratory droplets and can remain airborne in a room for up to two hours after an infected person has left. For the vast majority of vaccinated individuals, two doses of the measles-mumps-rubella (MMR) vaccine confer approximately 97% protection. For unvaccinated populations — including infants too young to be immunized and individuals who are immunocompromised — the risks of severe complications, including pneumonia, encephalitis, and death, are substantially higher.
The scale of the current US outbreak has reignited urgent conversations about herd immunity thresholds, the erosion of public trust in vaccines, and the responsibilities of public health leadership.
Current Situation
 Image: Pexels/Atypeek Dgn
Image: Pexels/Atypeek Dgn
According to reporting by the Center for Infectious Disease Research and Policy (CIDRAP), the US case total reached 1,714 infections as of the week ending April 10, 2026, reflecting a gain of 43 cases over the preceding seven days. That figure represented a meaningful deceleration from earlier in the outbreak, and a subsequent update covering the week of April 17 brought further encouraging news: only 34 new infections were recorded nationally, the smallest single-week increase reported so far this year.
While any downward trend in case counts is significant, epidemiologists caution against premature optimism. Weekly fluctuations in reported case numbers can reflect reporting lags, changes in testing access, or transient dips that precede renewed spread, rather than true outbreak control. Sustained reductions over multiple consecutive weeks are the more reliable signal that an outbreak is genuinely contracting.
Death toll data has not been centrally reported in these updates. Measles carries a case fatality rate in high-income countries of roughly 1–2 per 1,000 cases, though this rises sharply in populations with poor nutritional status or limited healthcare access. Hospitalizations and severe complications have been documented throughout this outbreak, though aggregate national figures have not been publicly released in the sources reviewed here.
Affected Regions
Utah has emerged as the single most active outbreak location in the United States. As of mid-April 2026, the state had recorded more than 600 confirmed measles cases, surpassing other outbreak zones and earning the designation as the country’s primary epicenter. Utah health officials reported 24 new cases in a five-day window in early April alone — a pace that underscores how rapidly the virus can move through under-vaccinated communities once it gains a foothold.
South Carolina, which had previously been among the more active outbreak states, showed a markedly different trajectory. Officials there reported no new cases during the same reporting period, suggesting that transmission chains may have been interrupted — either through vaccination catch-up efforts, natural depletion of susceptible individuals in affected communities, or both.
The broader US outbreak remains geographically dispersed. Measles does not respect state lines, and communities with pockets of unvaccinated individuals — regardless of geography — remain at elevated risk. Schools, religious communities with vaccine hesitancy, and international travel hubs are historically the environments where measles establishes and sustains transmission.
Risk Assessment
The greatest vulnerability in the current outbreak lies in communities where childhood MMR vaccination rates have fallen below the 95% coverage threshold required to sustain herd immunity — even a modest gap in coverage can allow measles to circulate widely among susceptible individuals.The populations at highest risk include unvaccinated or incompletely vaccinated children, infants under 12 months of age who are not yet eligible for the MMR vaccine, pregnant individuals (for whom measles can trigger premature labor and severe illness), and adults who received only a single vaccine dose under older guidelines or who were vaccinated with an older formulation prior to 1968 that provided incomplete protection.
Measles also poses a longer-term immunological risk through a phenomenon known as immune amnesia: infection can suppress existing immunity to other pathogens for months to years after recovery, effectively stripping individuals of previously acquired protections against unrelated diseases.
The rapid emergence of Utah as the national epicenter reflects the dynamics common to measles outbreaks globally — once introduced into a concentrated susceptible population, the virus amplifies quickly. WHO global surveillance data has reinforced the stakes: the organization has noted that millions of lives have been saved across Africa through sustained measles vaccination programs, a figure that underlines what becomes possible when immunization coverage collapses.
Prevention & Response
 Image: Pexels/Jvalenciazz Jhon
Image: Pexels/Jvalenciazz Jhon
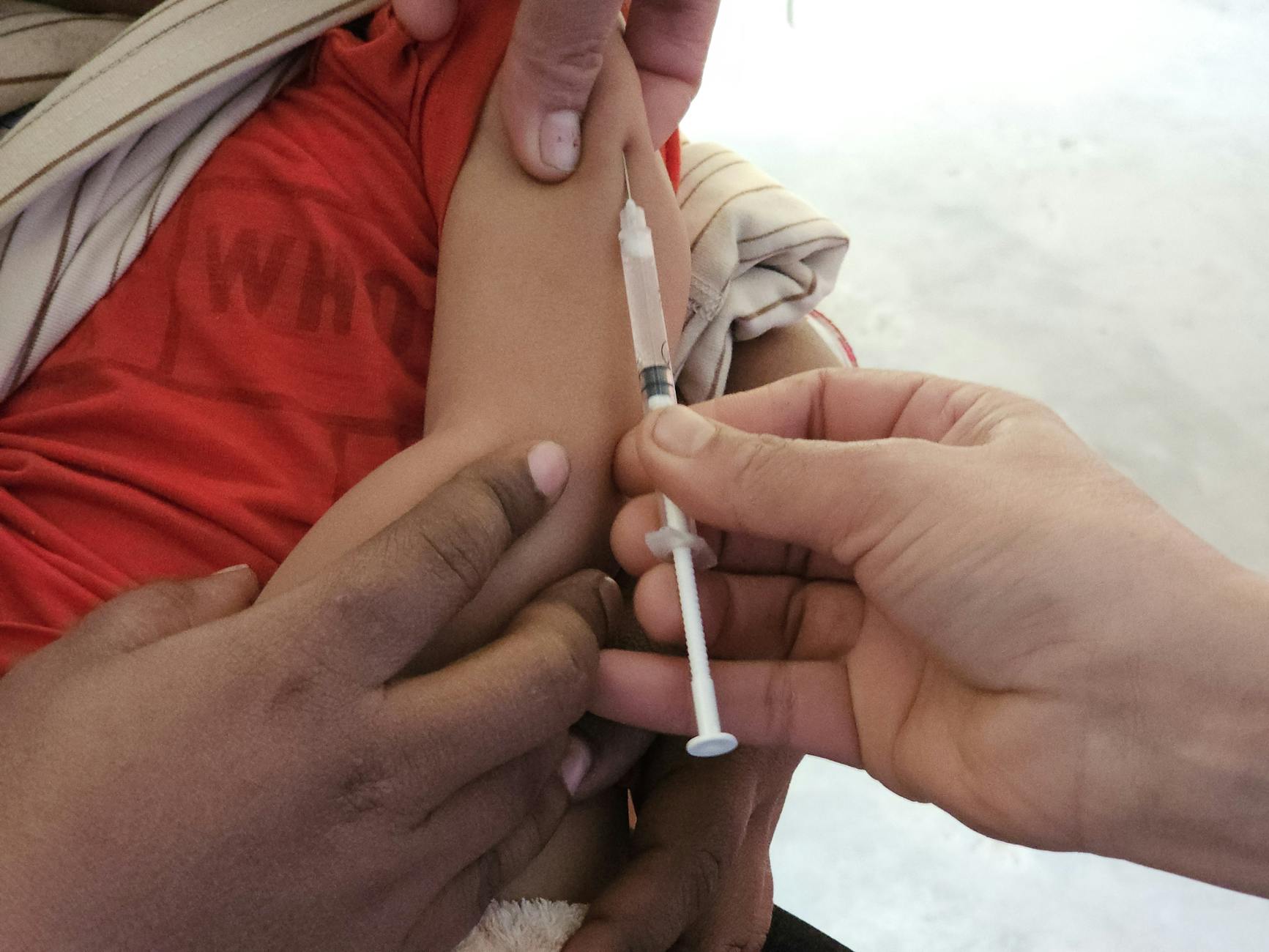
The primary tool for ending this outbreak is the same one that eliminated endemic measles transmission from the United States in 2000: the MMR vaccine. Public health officials have consistently reiterated that two doses, administered on the recommended schedule (the first at 12–15 months, the second at 4–6 years), remain highly effective and safe. Adults who are uncertain about their vaccination history can receive the MMR vaccine without harm.
The response has been complicated by persistent and, in some cases, high-profile misinformation about the vaccine’s composition and safety. HHS Secretary Robert F. Kennedy Jr. appeared before a House committee over two days in mid-April, defending his public health record and asserting that he has “never been anti-vaccine.” His testimony came amid scrutiny over statements attributed to him and other public figures regarding the MMR vaccine — including false claims that the vaccine contains “millions of particles” from aborted fetal tissue and millions of DNA fragments. A CIDRAP editorial addressing these claims directly found them to be without factual basis. The MMR vaccine does use cell lines derived from fetal tissue collected decades ago during legally performed procedures, but it contains no fetal tissue itself, and the quantities of residual DNA present are far below any established safety threshold.
Clinicians have also emphasized the practical importance of helping the general public distinguish measles from other febrile illnesses — particularly influenza, which shares some early symptoms. Measles typically begins with high fever, cough, runny nose, and conjunctivitis, followed by the appearance of Koplik’s spots (small white lesions inside the cheeks) and the characteristic red rash that spreads from the face downward across the body. Anyone suspecting measles exposure or infection is advised to call ahead before visiting a healthcare facility to prevent inadvertent spread in waiting rooms.
At the federal and state levels, outbreak response has included vaccination outreach, contact tracing in affected communities, and public communication campaigns. Whether these efforts will be sufficient to bring the outbreak fully under control depends in large part on the pace at which susceptible individuals seek vaccination — and on whether public confidence in the MMR vaccine can be maintained in the face of ongoing misinformation.
The tentative signs of slowing are meaningful. But with more than 1,700 Americans infected in a matter of months by a disease that was considered eliminated from this country a generation ago, the outbreak remains a stark illustration of what becomes possible when vaccination coverage erodes.
Sources
- CIDRAP. US measles total surpasses 1,700 cases. April 10, 2026.
- CIDRAP. US measles outbreak shows signs of slowing as WHO notes millions of lives saved in Africa by vaccination. April 17, 2026.
- CIDRAP. Utah measles outbreak tops 600 cases, now most active in the US. April 15, 2026.
- CIDRAP. South Carolina sees no new measles activity as Utah becomes epicenter of US outbreaks. April 8, 2026.
- CIDRAP. Kennedy defends measles record: ‘I have never been anti-vaccine.’ April 17, 2026.
- CIDRAP Op-Ed. Measles, misinformation, and what’s actually in the MMR vaccine. April 16, 2026.
- CIDRAP. Are your symptoms caused by the flu or measles? What to do before going to the doctor. April 10, 2026.